Guest, Staff &
Multi-Tenant WiFi.
The all-in-one platform for secure, compliant, and revenue-generating WiFi.
Trusted by the world's biggest brands







The all-in-one WiFi platform

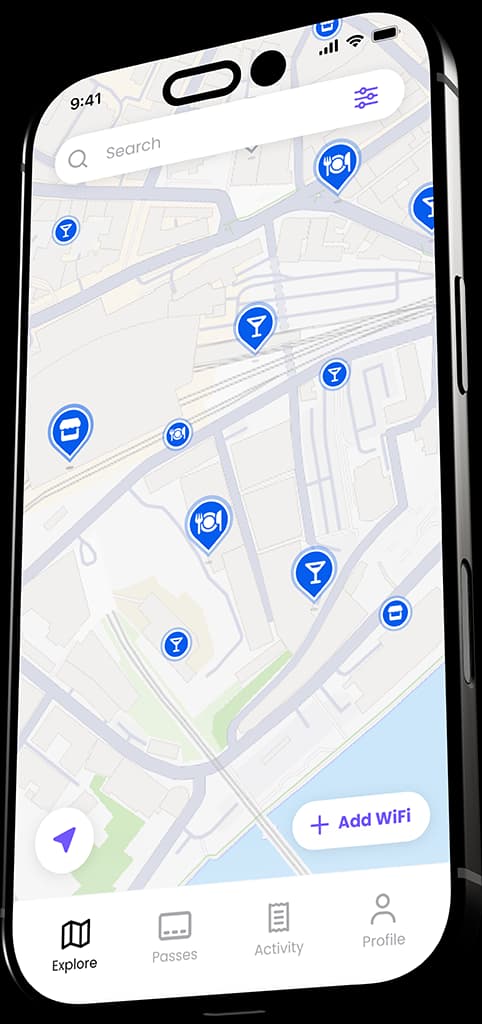
Engage with your guests
Capture visitor data, gain powerful analytics, and drive loyalty with our all-in-one guest WiFi platform.
- Branded captive portal or seamless connection
- Visitor analytics & reporting
- Marketing automation

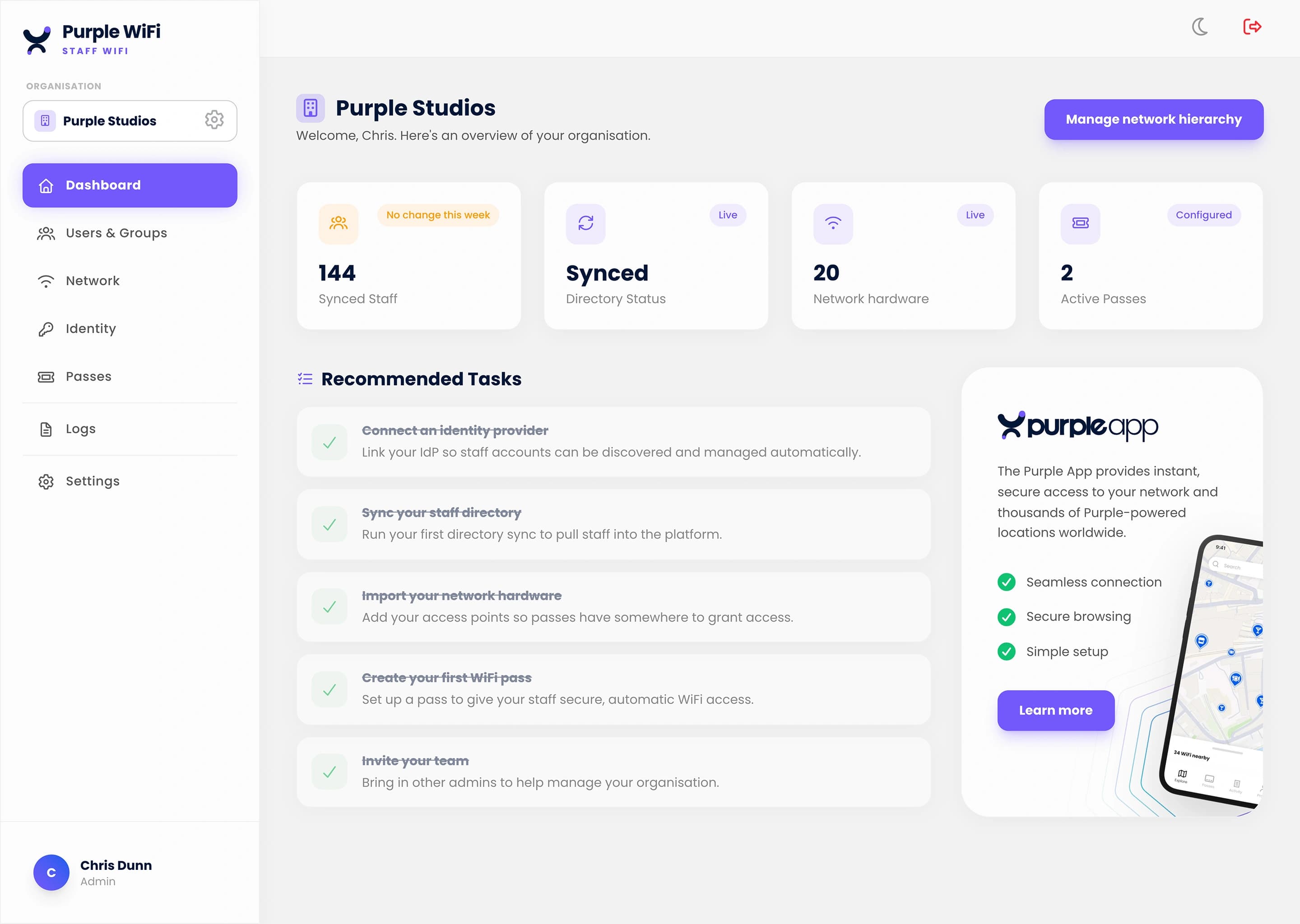
Passwordless zero trust
Effortlessly onboard employee devices with certificate-based authentication for secure, compliant network access.
- Works with Entra ID, Google, Okta
- Network segmentation
- Auto-revocation for JML

The at-home experience
Secure personal bubbles for all residents, for all their connected devices including browserless devices like consoles & TVs.
- Secure isolation from other guests
- iPSK for easy device connection
- Seamless connection upon return
Get started in three simple steps
Purple works with your existing hardware and infrastructure — a fully branded portal, live in minutes.
Connect your hardware
Purple is compatible with a wide range of hardware, including Cisco, Meraki, and Aruba.
Customize your portal
Design a branded captive portal with your logo, colors, and login options to match your venue's look and feel.
Go live
Once you're happy with your setup, simply go live and start collecting valuable visitor data.
What our customers are saying
Purple's solution is integral to our overall business strategies - not only does it allow us to tailor the user's journey based on individual venues, but it also allows us to collect valuable, rich data that would otherwise have been unknown to the business. This allows us to drive visits with tailored communications, which ultimately leads to an ROI that pays for the software itself, and then some!

Compared to the other platforms we looked at, Purple is more robust, the reports are impressive and the portal is far more visually appealing and easy to understand. The automated emails are good for saving time, allowing us to focus on planning new marketing campaigns.

The feedback that we have received from patients about the WiFi has been very positive, the weekly KPIs that we receive from Purple’s portal prove that the offering is well used and the user demographics have proved particularly interesting. Our main demographic at the hospital is elderly patients and in initial discussions about WiFi many people believed that this age category wouldn’t use the service. However, this has not been the case as many of our older patients use it. This information is useful to justify the usage amongst our largest demographic
We’re excited to be utilising Purple to enrich our charity communications mix. It’ll allow us to raise awareness of charity initiatives and increase the reach of our mailing list whilst providing secure, accessible and free WiFi to patients and visitors.
This state-of-the-art system will not only improve the experience of patients visiting Croydon University Hospital by reducing the stresses that navigating a large site can cause, but will also help them plot the quickest route to their care or to the loved ones they are visiting.
It’s a delight to work with Purple. The focus on delivering value to your customers is very apparent and nothing is too much trouble. Engagement is quick and sessions are always rewarding, ensuring we can continue to grow, to help provide the best possible service to our passengers
I’ve never had a supplier who so thoroughly understands our needs and objectives. Purple showed a very intricate understanding of the ticket sales model and that the use of an on-board portal was critical in reaching that huge untapped base!
Purple has provided a platform that has helped us achieve our goal of elevating the fan experience.
With the implementation of Purple’s tools, we are now able to offer a high-quality service to our passengers while gathering insights that allow us to understand the needs and expectations of our different passenger profiles and thus be able to identify concrete actions to improve the customer experience.
We are continually looking for new ways to enhance the customer experience, and Purple has helped us do just that, with the added benefit of customer insight
Purple knows their tech but it’s their people and their dedication to their jobs and professionalism that stand out. They understand that digital wayfinding in a healthcare environment is more than just downloading a mobile app.
Purple has been a fantastic partner! They are always excited to support our business objectives and quick to respond to any emails/requests we may have enabling us to deliver against our organisational goals.
Purple has provided a gateway for us to begin building better customer profiles
Purple's solution is integral to our overall business strategies - not only does it allow us to tailor the user's journey based on individual venues, but it also allows us to collect valuable, rich data that would otherwise have been unknown to the business. This allows us to drive visits with tailored communications, which ultimately leads to an ROI that pays for the software itself, and then some!
Compared to the other platforms we looked at, Purple is more robust, the reports are impressive and the portal is far more visually appealing and easy to understand. The automated emails are good for saving time, allowing us to focus on planning new marketing campaigns.
The feedback that we have received from patients about the WiFi has been very positive, the weekly KPIs that we receive from Purple’s portal prove that the offering is well used and the user demographics have proved particularly interesting. Our main demographic at the hospital is elderly patients and in initial discussions about WiFi many people believed that this age category wouldn’t use the service. However, this has not been the case as many of our older patients use it. This information is useful to justify the usage amongst our largest demographic
We’re excited to be utilising Purple to enrich our charity communications mix. It’ll allow us to raise awareness of charity initiatives and increase the reach of our mailing list whilst providing secure, accessible and free WiFi to patients and visitors.
This state-of-the-art system will not only improve the experience of patients visiting Croydon University Hospital by reducing the stresses that navigating a large site can cause, but will also help them plot the quickest route to their care or to the loved ones they are visiting.
It’s a delight to work with Purple. The focus on delivering value to your customers is very apparent and nothing is too much trouble. Engagement is quick and sessions are always rewarding, ensuring we can continue to grow, to help provide the best possible service to our passengers
I’ve never had a supplier who so thoroughly understands our needs and objectives. Purple showed a very intricate understanding of the ticket sales model and that the use of an on-board portal was critical in reaching that huge untapped base!
Purple has provided a platform that has helped us achieve our goal of elevating the fan experience.
With the implementation of Purple’s tools, we are now able to offer a high-quality service to our passengers while gathering insights that allow us to understand the needs and expectations of our different passenger profiles and thus be able to identify concrete actions to improve the customer experience.
We are continually looking for new ways to enhance the customer experience, and Purple has helped us do just that, with the added benefit of customer insight
Purple knows their tech but it’s their people and their dedication to their jobs and professionalism that stand out. They understand that digital wayfinding in a healthcare environment is more than just downloading a mobile app.
Purple has been a fantastic partner! They are always excited to support our business objectives and quick to respond to any emails/requests we may have enabling us to deliver against our organisational goals.
Purple has provided a gateway for us to begin building better customer profiles
Purple's solution is integral to our overall business strategies - not only does it allow us to tailor the user's journey based on individual venues, but it also allows us to collect valuable, rich data that would otherwise have been unknown to the business. This allows us to drive visits with tailored communications, which ultimately leads to an ROI that pays for the software itself, and then some!
Compared to the other platforms we looked at, Purple is more robust, the reports are impressive and the portal is far more visually appealing and easy to understand. The automated emails are good for saving time, allowing us to focus on planning new marketing campaigns.
The feedback that we have received from patients about the WiFi has been very positive, the weekly KPIs that we receive from Purple’s portal prove that the offering is well used and the user demographics have proved particularly interesting. Our main demographic at the hospital is elderly patients and in initial discussions about WiFi many people believed that this age category wouldn’t use the service. However, this has not been the case as many of our older patients use it. This information is useful to justify the usage amongst our largest demographic
We’re excited to be utilising Purple to enrich our charity communications mix. It’ll allow us to raise awareness of charity initiatives and increase the reach of our mailing list whilst providing secure, accessible and free WiFi to patients and visitors.
This state-of-the-art system will not only improve the experience of patients visiting Croydon University Hospital by reducing the stresses that navigating a large site can cause, but will also help them plot the quickest route to their care or to the loved ones they are visiting.
It’s a delight to work with Purple. The focus on delivering value to your customers is very apparent and nothing is too much trouble. Engagement is quick and sessions are always rewarding, ensuring we can continue to grow, to help provide the best possible service to our passengers
I’ve never had a supplier who so thoroughly understands our needs and objectives. Purple showed a very intricate understanding of the ticket sales model and that the use of an on-board portal was critical in reaching that huge untapped base!
Purple has provided a platform that has helped us achieve our goal of elevating the fan experience.
With the implementation of Purple’s tools, we are now able to offer a high-quality service to our passengers while gathering insights that allow us to understand the needs and expectations of our different passenger profiles and thus be able to identify concrete actions to improve the customer experience.
We are continually looking for new ways to enhance the customer experience, and Purple has helped us do just that, with the added benefit of customer insight
Purple knows their tech but it’s their people and their dedication to their jobs and professionalism that stand out. They understand that digital wayfinding in a healthcare environment is more than just downloading a mobile app.
Purple has been a fantastic partner! They are always excited to support our business objectives and quick to respond to any emails/requests we may have enabling us to deliver against our organisational goals.
Purple has provided a gateway for us to begin building better customer profiles
Ready to fix your WiFi?
Speak to one of our experts to find out how Purple can help you transform your venue's WiFi experience.